Aortic Stenosis and Transcatheter Aortic Valve Replacement (TAVR / TAVI)- The aortic valve is the most important of the four heart valves that control the flow of blood in and out of the heart. If the aortic valve becomes abnormally narrow (aortic stenosis) or leaks (aortic regurgitation), the heart must work harder to pump the same amount of blood. As a result, the heart muscle thickens, and the chambers of the heart may enlarge and ultimately lead to heart failure.
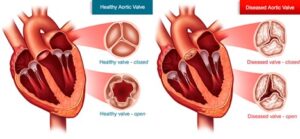
If aortic valve disease is left untreated, it leads to breathlessness, chest pain, blackouts, heart failure and eventually death.
In patients with severe aortic stenosis, the only effective long-term treatment is to replace the valve.
Transcatheter Aortic Valve Replacement (TAVR / TAVI)
Transcatheter aortic valve implantation (TAVI) or replacement (TAVR) is a minimally invasive procedure that involves inserting a catheter into a blood vessel in your upper leg and passing it towards your native aortic valve to implant a new valve.
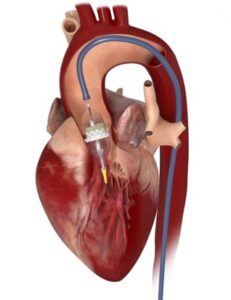
Under local anaesthetic, a small tube called a sheath will be inserted in the artery at the top of one of your legs or arm for taking pictures during the procedure. A slightly bigger sheath will be inserted into the artery at the top of your other leg, which the new valve will go through. Sometimes, a temporary pacemaker will be put into your heart through a vein in your neck or leg in case the doctor needs to speed up your heart during the procedure.
Catheters (small tubes) are passed through the bigger sheath to pass a long ‘guide wire’ across the narrowed aortic valve. The new aortic valve is then advanced over this wire (like a train on rail tracks) until it is in place inside your narrowed valve and then expanded to push the narrowed valve open, creating a new valve within it. A small balloon (‘balloon catheter’) may be used to widen your narrowed aortic valve before the new aortic valve is placed. It may also be used to widen the new aortic valve after it has been implanted.
It is a low risk minimally invasive procedure with quick recovery and short hospital stay.
The main advantages of this technique are that the heart doesn’t need to be stopped, so a heart-lung (bypass) machine doesn’t need to be used, and it avoids making a large cut (incision) in your chest. This puts less strain on the body and may mean TAVI is more suitable for people who are at high risk to have a conventional valve replacement or need a quick recovery with shorter hospital stay.